Was sind Blutungsstörungen / Zyklusstörungen?
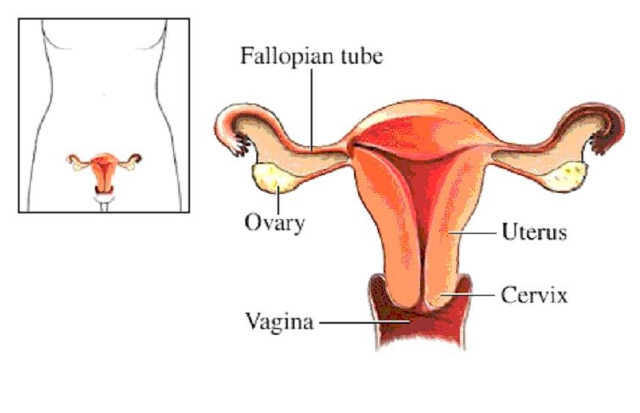
Die Organe und Strukturen des reproduktiven Systems
- Die Gebärmutter ist ein birnenförmiges Organ, das sich zwischen der Blase und dem unteren Darm befindet. Es besteht aus zwei Teilen, dem Körper und dem Gebärmutterhals.
- Ist eine Frau nicht schwanger, ist der Gebärmutterkörper etwa so groß wie eine Faust, und die Wände sind zusammengefaltet und gegeneinander abgeflacht. Während der Schwangerschaft werden die Wände der Gebärmutter auseinandergedrückt, wenn der Fötus wächst.
- Der Gebärmutterhals ist der untere Teil der Gebärmutter. Es hat einen Kanal, der in die Vagina mündet, mit einer Öffnung, die als Os bezeichnet wird und es dem Menstruationsblut ermöglicht, aus der Gebärmutter in die Vagina zu fließen.
- Von jeder Seite des Gebärmutterkörpers führt ein röhrenförmiger Kanal, der als Eileiter Eileiter bezeichnet wird. Nahe dem Ende jeden Eileiters befindet sich ein Eierstock.
- Die Eierstöcke sind eierzeugende Organe, die zwischen 200.000 und 400.000 Follikel enthalten (aus Folliculus, was lateinisch „Sack“ bedeutet). Diese Zellensäcke enthalten die Materialien, die zur Herstellung gereifter Eier oder Eizellen benötigt werden.
- Die innere Gebärmutterschleimhaut wird Endometrium genannt. Während der Schwangerschaft verdickt sie sich und wird mit Blutgefäßen angereichert, um den wachsenden Fötus aufzunehmen und zu unterstützen. Wenn keine Schwangerschaft eintritt, wird das Endometrium als Teil des Menstruations-flusses abgestoßen. Der Menstruationsfluss besteht auch aus Blut und Schleim aus dem Gebärmutterhals und der Vagina.
Was ist eine Menorrhagie ?
During normal menstruation the average woman loses about 2 ounces (60 ml) of blood or less.
If bleeding is significantly heavier, it is called menorrhagia, which occurs in 9% to 14% of all women and can be caused by a number of factors.
Women often over estimate the amount of blood lost during their periods.
However, women should consult their physician if any of the following occurs:
- Soaking through at least one pad or tampon every hour for several hours.
- Heavy periods that regularly lasting 10 or more days.
- Bleeding between periods or during pregnancy.
- Spotting or light bleeding between periods is common in girls just starting menstruation and sometimes during ovulation in young adult women, but consultation with a physician is nevertheless recommended.
Note: Clot formation is fairly common during heavy bleeding and is not a cause for concern.
Ursachen für verstärkte Gebärmutterblutungen
Almost all women, at some time in their reproductive life, experience heavy bleeding during a period.
Each year, up to 2 million women consult their physicians about menorrhagia.
It is the most common gynecologic complaint and the reason for two-thirds of all hysterectomies.
A number of conditions can cause menorrhagia or contribute to the risk, although often the cause of heavy bleeding is unknown.
In fact, no abnormalities to explain the bleeding are detected in about half of hysterectomies performed because of menorrhagia.
It should be pointed out, however, that while up to 30% of premenopausal women complain of heavy bleeding, only 10% experience blood loss severe enough to be defined as menorrhagia. (On the other hand, some women might have menorrhagia but think it is normal. Such women are likely to have a family history of bleeding disorders and so believe that a heavy period is natural. )
With normal menstruation women lose about 2 ounces (60 ml) of blood or less.
Factors Associated with a Higher Risk for Heavy Menstrual Bleeding
Certain characteristics are associated with a higher risk for menorrhagia:
- Being taller.
- Being older. (Women who are approaching menopause may experience occasional menorrhagia.)
- Having a higher number of pregnancies.
DYSFUNCTIONAL UTERINE BLEEDING
Dysfunctional uterine bleeding (DUB) is a general term for abnormal bleeding caused by hormonal abnormalities and is one of the primary causes of menorrhagia.
In many cases, DUB occurs either when a girl just starting to menstruate or as women approach menopause, but it can occur at any time in during a woman’s reproductive life.
ANOVULATORY DUB.
About 90% of DUB events occur when ovulation is not occurring (anovulatory DUB).
In such cases, follicles do not properly develop and release a mature egg.
When this happens, the corpus luteum, which is a mound of tissue that produces progesterone, does not form.
As a result, estrogen is produced continuously, causing an overgrowth of the uterus lining.
The period is delayed in such cases, and when it occurs menstruation can be very heavy and prolonged.
Sometimes anovulatory DUB is due to a delay in the full maturation of the reproductive system in teenagers.
Usually, however, the mechanisms are unknown.
OVULATORY DUB.
The other 10% of cases occur in women who are ovulating, but progesterone secretion is prolonged because estrogen levels are low.
This causes irregular shedding of the uterine lining and break-through bleeding.
Some evidence has associated ovulatory DUB with more fragile blood vessels in the uterus.
OTHER CAUSES OF MENORRHAGIA
Uterine Fibroids
Fibroids are the other important known causes of heavy menstrual bleeding
FOR MORE DETAILS CLICK THE LINK BELOW
http://www.endogyn.de/index.php?seite=endogyn&sprache=en&a=Specialtreatments&b=Fibroids
Von Willebrand Disease and Other Bleeding Disorders
Bleeding disorders that impair blood clotting can cause heavy menstrual bleeding and, according to different studies, have been associated with between 10% and 17% of menorrhagia cases.
Von Willebrand disease, a genetic condition, is the most common of these bleeding disorders and may be underdiagnosed in many women with unexplained menorrhagia.
Most studies, report this problem to be more common in African American than Caucasian women.
Other rare disorders that impair blood platelets and clotting factors can also account for some cases of menorrhagia.
Most bleeding disorders have a genetic basis and should be suspected in adolescent girls who experience heavy bleeding.
Abnormal Blood Vessel Growth
Every month, blood vessels regrow in the uterus to replace the blood-rich uterine lining lost during menstruation.
Abnormalities in this growth process (called arteriogenesis or angiogenesis) may occur in some women with menorrhagia.
Some research indicates that imbalances in certain immune factors and growth hormones can affect angiogenesis and may be responsible for some cases of menorrhagia.
Abnormalities in the Uterus
Structural problems or other abnormalities in the uterus may cause bleeding.
They include the following.
- Miscarriage. An isolated instance of heavy bleeding usually after the period due date may be due to a miscarriage. If the bleeding occurs at the usual time of menstruation, however, miscarriage is less likely to be a cause.
- Uterine polyps. (These are small benign growths in the uterus.)
- Adenomyosis. This condition occurs when glands from the uterine lining become embedded in the uterine muscle. Its symptoms are nearly identical to fibroids (heavy bleeding and pain). Heavy bleeding occurs in between 36% and 70% of cases. It is most likely to develop in middle-aged women who have had many children.
- Endometriosis. (These are small implants of uterine tissue. They are more likely to cause pain than bleeding.)
- Uterine cancer.
- Infections or inflammation in the vagina, service, or pelvic area.
Other Medical Conditions or Medications That Cause Heavy Menstrual Bleeding
- Certain medical disorders and drugs increase the risk for heavy bleeding.
- Medical conditions that may increase the risk for menorrhagia include thyroid problems, systemic lupus erythematosus, diabetes, and certain cancers and chemotherapies.
- Certain drugs, including anticoagulants and anti-inflammatory medications, can cause heavy bleeding.
- Some contraceptives, including certain oral contraceptives or the Copper T intrauterine device–an IUD, may also pose a risk for heavy bleeding. It should be noted, however, that some oral contraceptives and the progesterone-releasing IUD can be used to stop bleeding.
Einleitung
Jedes Jahr wird in Deutschland bei ca. 160.000 Frauen die Gebärmutter entfernt (Hysterektomie). In mehr als 80% der Fälle kommt es zur Hysterektomie auf Grund von Störungen in der Monatsblutung, Myomen oder einfach, weil die Gebärmutter vergrößert ist. Für ein Drittel bis zur Hälfte der Patientinnen wäre eine weniger invasive Operationstechnik einsetzbar. Vielfach gibt es keinen Grund, übereilt einer Hysterektomie zuzustimmen. Mehr denn je ist es ratsam, sich zuerst einmal Informationen zu beschaffen und die Vor- und Nachteile einer Gebärmutterentfernung sorgfältig abzuwägen.
Störungen der Monatsblutung
Die Gebärmutter ist ein birnenförmiges, muskuläres Hohlorgan mit einer typischen Länge zwischen sieben und neun Zentimetern. Sie ist innen mit einer Schleimhautschicht ausgekleidet, dem Endometrium, in welcher sich im Falle einer Schwangerschaft das befruchtete Ei einnisten kann. Liegt keine Schwangerschaft vor, wird die Schleimhautschicht ca. alle 28 Tage erneuert. Mindestens eine von fünf Frauen im Alter zwischen 35 und 50 Jahren leidet an schweren und verlängerten Monatsblutungen, zudem oft einher gehend mit heftigen vormenstruellen Beschwerden. Diese können ihre Ursache haben in hormonellen Schwankungen vor oder während der Menopause, gutartigen Wucherungen in der Gebärmutter (Polypen, Myome), bestimmten Infektionen aber auch in chronischen Erkrankungen. Die hiervon betroffenen Frauen weisen Symptome auf, wie beispielsweise starke und unkontrollierbare Blutungen, heftige Krämpfe im Unterleib, Anämie, Brechreiz, Müdigkeit und eine verringerte Lebenskraft. Ihre Lebensqualität ist beeinträchtigt. In solchen Fällen betrachten sich die Frauen häufig als „nicht vorzeigbar“ und ziehen sich in sich zurück. Sie schränken ihre Aktivitäten ein, was wiederum negative Auswirkungen auf das Berufs- und Familienleben hat.
Wann sollte die Gebärmutter entfernt werden?
Für Frauen jenseits der 40 ist die Hysterektomie nach wie vor die populärste Therapieform bei Störungen oder Beschwerden an diesem Organ. Die völlige Entfernung der Gebärmutter hat tiefgehende Auswirkungen für die Frauen und führt oft zu körperlichen oder seelischen Belastungen. Daher sollte die Entscheidung für eine Hysterektomie sorgfältig abgewogen werden. Eine Operation ist jedoch immer dann unausweichlich, wenn Vorstufen von Krebs oder Krebs diagnostiziert werden. Diese zwingenden Indikationen gelten jedoch nur in ca. 20% der Behandlungsfälle.
Die Behandlung von Blutungsstörungen
Für den Fall von Blutungsstörungen, die auf keine hormonelle Behandlung oder Ausschabung ansprechen wird häufig die Gebärmutterentfernung als die einzig Erfolg versprechende Maßnahme angesehen. In den meisten Fällen könnte jedoch das Organ erhalten bleiben, kämen moderne, weniger invasive Methoden zum Einsatz. So wird beispielsweise bei einem als Endometriumablation oder –koagulation bezeichneten Verfahren nur die Gebärmutterschleimhaut und eine dünne Schicht von Muskelgewebe durch Hitzebehandlung verödet. Der Eingriff erfolgt über die natürliche Öffnung der Gebärmutter. Hierzu existieren mehrere Methoden: elektrochirurgische Instrumente, Heißwasserballons sowie Hochfrequenz- und Mikrowellenchirurgie. Nach der Behandlung wird die Gebärmutterschleimhaut vom Körper ausgestoßen. Danach kommt es zu keinen bis geringen Monatsblutungen. Diese Behandlungsformen können in einer Tagesklinik unter kurzer Vollnarkose durchgeführt werden. Es ist unbedingt darauf zu achten, dass keine malignen Veränderungen der Gebärmutterschleimhaut vorliegen und dass die Patientin mit der Familienplanung abgeschlossen hat.
(Quelle: Ein Beitrag von Dr. Kruschinski in der ZDF Sendung „Ratgeber Gesundheit)
REPRODUCTIVE HORMONES.
The hypothalamus (an area in the brain) and the pituitary gland regulate the reproductive hormones.
The pituitary gland is often referred to as the master gland because of its important role in many vital functions, many of which require hormones.
In women, six key hormones serve as chemical messengers that regulate the reproductive system:
- The hypothalamus first releases the gonadotropin-releasing hormone (GnRH).
- This chemical, in turn, stimulates the pituitary gland to produce follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
- Estrogen, progesterone, and the male hormone testosterone are secreted by the ovaries at the command of FSH and LH and complete the hormonal group necessary for reproductive health.
OVULATION.
The process leading to fertility is very intricate. It depends on the healthy interaction of two sets of organs and hormone systems in both the male and female. In addition, reproduction is limited by the phases of female fertility. Nevertheless, this astonishing process results in conception within a year for about 80% of couples. Only 15% conceive within a month of their first attempts, however, and about 60% succeed after six months.
A woman’s ability to produce children occurs after she enters puberty and begins to menstruate.
The process to conception is complex:
- With the start of each menstrual cycle, follicle-stimulating hormone (FSH) stimulates several follicles to mature over a two-week period until their eggs nearly triple in size.
- Only one follicle becomes dominant, however, during a cycle.
- FSH signals this dominant follicle to produce estrogen, which enters the bloodstream and reaches the uterus.
- There, estrogen stimulates the cells in the uterine lining to reproduce, therefore thickening the walls.
- Estrogen levels reach their peak around the 14th day of the cycle (counting days beginning with the first day of a period).
- At that time, they trigger a surge of luteinizing hormone (LH).
LH serves two important roles:
- First, the LH surge around the 14th cycle day stimulates ovulation. It does this by causing the dominant follicle to burst and release its egg into one of the two fallopian tubes. Once in the fallopian tube, the egg is in place for fertilization.
- Next, LH causes the ruptured follicle to develop into the corpus luteum. The corpus luteum provides a source of estrogen and progesterone during pregnancy.
FERTILIZATION.
The so-called „fertile window“ is six days long and starts five days before ovulation and ends the day of ovulation.
Fertilization occurs as follows:
- The sperm can survive for up to three days once it enters the fallopian tube.
- The egg survives 12 to 24 hours unless it is fertilized by a sperm.
- If the egg is fertilized, about two to four days later it moves from the fallopian tube into the uterus where it is implanted in the uterine lining and begins its nine-month incubation.
- The placenta forms at the site of the implantation. The placenta is a thick blanket of blood vessels that nourishes the fertilized egg as it develops.
- The corpus luteum (the yellow tissue formed from the ruptured follicle) continues to produce estrogen and progesterone during pregnancy.
- If the egg is not fertilized, the corpus luteum degenerates into a form called the corpus albicans, and estrogen and progesterone levels drop.
- Finally, the endometrial lining sloughs off and is shed during menstruation.